

Product Specifications
- Peptide: Sermorelin
- Other Designations: GRF 1-29, GHRH (1-29)-amide, Growth Hormone-Releasing Factor (1-29) amide
- Classification: Growth Hormone-Releasing Hormone (GHRH) Analog
- Available Size: 5mg
- Form: Lyophilized (freeze-dried) powder
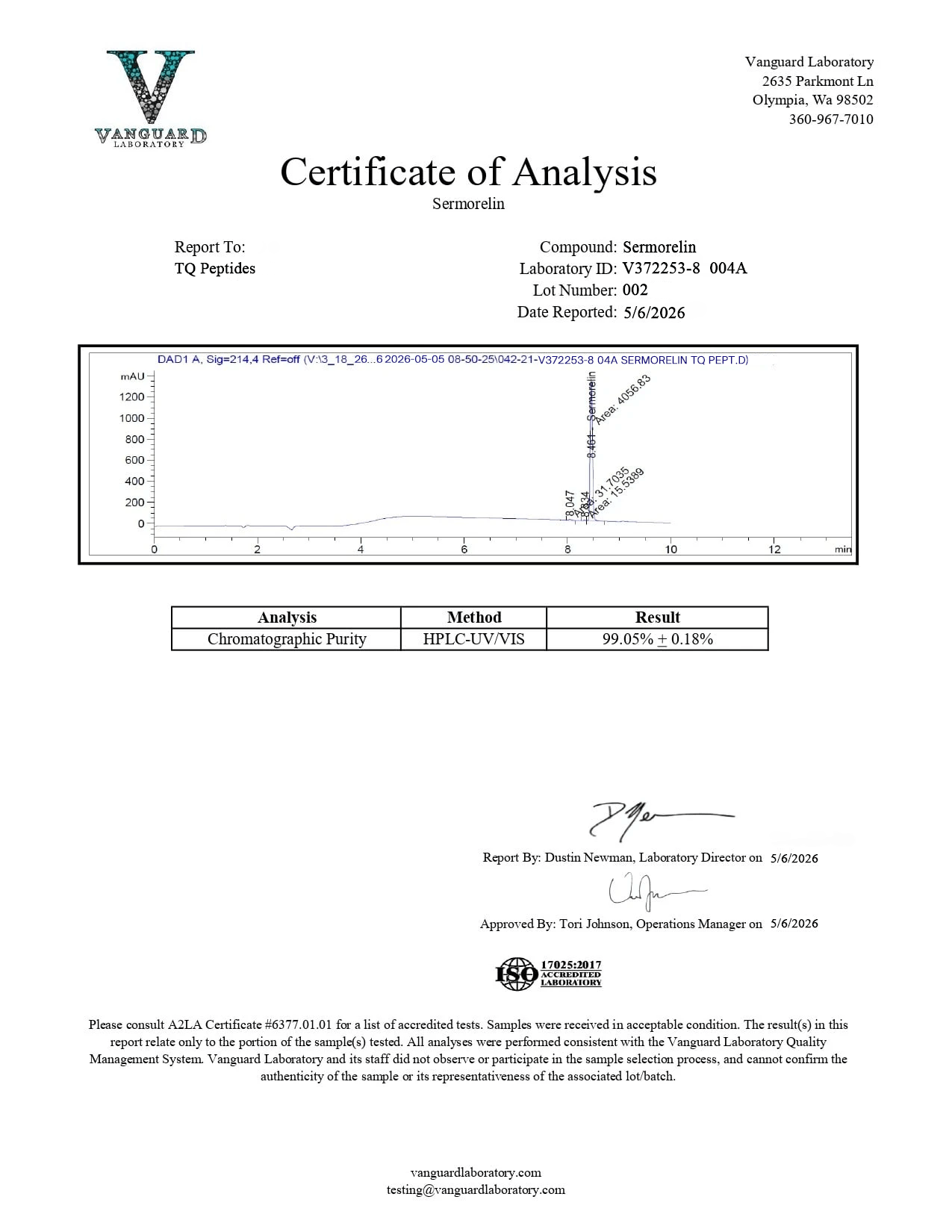
- Purity: >99%
- Amino Acid Count: 29
- Molecular Formula: C₁₄₉H₂₄₆N₄₄O₄₂S
- Molecular Weight: 3357.93 g/mol
- Half-Life: Approximately 11–12 minutes
- Receptor Target: Growth Hormone-Releasing Hormone Receptor (GHRH-R)
- Origin: Wholly synthetic — represents the first 29 amino acids of the 44-amino-acid native GHRH sequence
- Regulatory History: Previously FDA-approved for diagnostic use in growth hormone deficiency assessment
- Storage: Store lyophilized powder at -20°C. Once reconstituted, store at 2–8°C and use within 30 days.
- Intended Use: For laboratory and research professionals only. Not intended for human or veterinary consumption; use exclusively in controlled scientific studies.
- Third-party tested with Certificate of Analysis available.
What Is Sermorelin? (For Researchers and Lab Use Only)
Sermorelin is a synthetic peptide of 29 amino acids. It is the shortest functional fragment of human growth hormone-releasing hormone (GHRH), the endogenous 44-amino-acid hormone that stimulates growth hormone (GH) secretion from the anterior pituitary gland. Though it has only the first 29 amino acids of the native hormone’s 44, Sermorelin keeps full biological activity at the GHRH receptor. It is the minimal sequence needed to trigger physiological GH release.
Sermorelin has been studied since the early 1980s, when researchers showed that exogenous GHRH (1-29) amide could stimulate pituitary function and growth in animal models. Building on these findings, the peptide became an important research tool for the GH axis and was once FDA-approved as a diagnostic agent for growth hormone deficiency. Although its clinical status has changed, Sermorelin persists as one of the most studied GHRH analogs, with published research spanning growth, body composition, cognition, lipodystrophy, tumor biology, and reproductive endocrinology.
A defining feature of Sermorelin is its receptor specificity. It binds directly to the GHRH receptor, the same one activated by the body’s own GHRH. Sermorelin is reported to stimulate GH secretion without altering other endocrine markers, such as prolactin, insulin, cortisol, glucose, or thyroid hormones. This specificity makes Sermorelin a clean research tool for studying GH-mediated effects alone.
Sermorelin has a half-life of about 11–12 minutes, compared to native GHRH at around 7 minutes and modified analogs like CJC-1295 with DAC at 6–8 days. This intermediate value makes Sermorelin a pulse-format GHRH agonist, producing brief, time-limited GH secretion that closely mirrors the body’s natural pulsatile GH release pattern.
How Sermorelin Works — Proposed Mechanism of Action
Sermorelin is proposed to stimulate growth hormone release by binding to GHRH receptors on somatotroph cells in the anterior pituitary gland. This binding is believed to change the receptor’s shape. It then starts an intracellular signaling cascade with several steps:
Activation of the GHRH receptor signals a helper protein (Gs), which then activates the enzyme adenylate cyclase. Adenylate cyclase converts ATP into cAMP, an important signaling molecule within the cell.
As cAMP accumulates, it activates protein kinase A (PKA), an enzyme that transmits the signal through the cell.
Protein kinase A (PKA) then adds phosphate groups to target proteins, switching on genes responsible for growth hormone production. This results in the release of stored growth hormone from the cell into the body.
After release, growth hormone binds to its receptors on target tissues such as the liver, activating the JAK-STAT signaling pathway and stimulating the production of insulin-like growth factor 1 (IGF-1), which mediates cellular growth, protein synthesis, and tissue repair.
Sermorelin activates the same receptor and the same Gs/cAMP/PKA signaling pathway as CJC-1295, both with and without DAC. The main differences are in half-life and pharmacokinetics. Sermorelin produces brief, pulsatile GH release with a half-life of about 11–12 minutes. CJC-1295 without DAC produces longer pulses of about 30 minutes. CJC-1295 with DAC can elevate GH for several days (about 6–8 days). Researchers choose based on whether they want pulse-pattern, intermediate, or chronic GH-axis stimulation.
Sermorelin’s Position in the GHRH Analog Family
Understanding where Sermorelin fits in the broader GHRH analog landscape helps research professionals and laboratory scientists choose the right compound for their protocols and study designs.
- Native GHRH (1-44) — The full-length endogenous hormone. Half-life of approximately 7 minutes. Rapidly degraded by dipeptidyl peptidase-4 (DPP-IV). Rarely used in research due to extreme instability.
- Sermorelin or GRF 1-29 is the shortest functional GHRH fragment. It has a half-life of about 11–12 minutes and keeps full receptor activity. It was previously FDA-approved. Sermorelin is the most extensively studied GHRH analog and has the widest published research portfolio.
- CJC-1295 without DAC (Mod GRF 1-29) — A tetrasubstituted version of GRF 1-29 with four amino acid modifications for enhanced stability. Half-life of approximately 30 minutes. More resistant to enzymatic degradation than Sermorelin.
- CJC-1295 with DAC — The same tetrasubstituted backbone plus a Drug Affinity Complex for plasma protein binding. Half-life of approximately 6–8 days. Produces sustained, multi-day GH and IGF-1 elevation.
Sermorelin is unique among GHRH analogs. It is the most natural analog, and its structure is closest to endogenous GHRH. It is also the most studied in clinical settings. Sermorelin closely replicates physiological GH pulsatility. For researchers studying natural GH release patterns, Sermorelin remains the reference standard.
Preclinical and Clinical Research Overview
Sermorelin has been investigated across a remarkably diverse range of research domains. Below is a detailed summary organized by study focus.
Sermorelin and Growth Hormone Stimulation
The main effect of Sermorelin is to help the body produce more growth hormone. This has been measured in many clinical studies.
In one study, single nightly doses of Sermorelin in elderly subjects increased average growth hormone levels by 82%. The effect lasted for about 2 hours after administration. Another 16-week study reported Sermorelin may raise growth hormone levels by up to 107% and IGF-1 by about 28%. The same study found a gain of about 1.26 kg (2.78 lbs) in lean body mass, with no significant change in fat mass. Skin thickness also increased. The authors linked these results to the peptide’s ability to stimulate the GH/IGF-1 axis.
These results are consistent with the pulse-format pharmacokinetics of Sermorelin: repeated presentations producing cumulative anabolic effects through sequential, time-limited GH secretion events rather than the sustained elevation produced by longer-acting analogs.
Sermorelin and Growth Velocity in GH Deficiency
Sermorelin’s earliest and most established research application is in models of idiopathic growth hormone deficiency.
In studies involving growth-impaired subjects, regular Sermorelin administration led to measurable increases in growth velocity within 12 months. These higher growth rates lasted an average of 36 months when the peptide was continuously administered. The data suggest Sermorelin’s effects are not just an initial burst but can provide steady GH axis stimulation over long-term use.
This finding about sustained growth velocity is key. It addresses whether GHRH-analog-stimulated GH release persists over time or if the pituitary develops tolerance. The multi-year data suggest Sermorelin may keep the GH axis responsive without much desensitization.
Sermorelin and Lipodystrophy / Body Composition
One of the most clinically relevant areas of Sermorelin research focuses on body composition in subjects with HIV-associated lipodystrophy. This condition is characterized by abnormal fat redistribution, including excess fat in the abdomen and loss of fat in the limbs.
In a controlled clinical study involving 31 HIV-positive subjects with lipodystrophy, participants were divided into two groups: one receiving Sermorelin and the other receiving a placebo for 12 weeks. The investigators reported several notable findings:
- Growth hormone levels were significantly higher in the Sermorelin group than in the placebo group.
- IGF-1 levels reportedly increased, corresponding with increased lean body mass in the peptide group.
- Abdominal visceral fat and the ratio of trunk-to-lower-extremity fat appeared significantly reduced.
- No significant changes in glucose or insulin levels were observed.
The absence of changes in glucose and insulin is especially important. It supports Sermorelin’s receptor specificity. The peptide appeared to raise GH and IGF-1 without affecting metabolic markers that other hormonal treatments might change.
Sermorelin and Cognition
An intriguing line of Sermorelin research links declining growth hormone levels in aging populations to cognitive performance and investigates whether restoring GH secretion via GHRH receptor stimulation may influence cognitive function.
In a clinical study involving 89 subjects aged 68-69, researchers explored the hypothesis that age-related GH decline may contribute to impaired cognitive function—specifically, the ability to collect, process, and recall information. Following the Sermorelin presentation, investigators observed apparent improvements in performance on the Wechsler Adult Intelligence Scale (WAIS), including higher IQ scores, better performance on picture arrangement tests, and improved verbal assessments.
These findings are particularly notable because they suggest Sermorelin’s downstream effects may extend beyond the classically studied anabolic outcomes (body composition, growth velocity) into the domain of central nervous system function. The proposed mechanism — that restored GH and IGF-1 levels may support neural processes involved in cognition — represents an important area for further investigation, especially given the global research focus on age-related cognitive decline.
Sermorelin and Tumor Cell Research
In a study that departs from Sermorelin’s traditional GH-axis research profile, investigators examined the peptide’s potential interactions with tumor cell biology.
A large-scale clinical study design involved 1,018 glioma subjects, each of whom was presented with over 4,000 compounds. A drug response score (DRS) was calculated for each compound in each subject to identify those that induced the greatest tumor cell sensitivity. Among the 4,000+ compounds tested, Sermorelin reportedly yielded the highest sensitivity scores in glioma subjects.
Investigators proposed that this observation may be related to Sermorelin’s potential to interfere with tumor cell cycle progression — specifically by blocking cell cycle advancement and potentially preventing tumor cell proliferation. While the mechanism requires further investigation and confirmation, this finding positions Sermorelin as a compound of interest in oncological research, separate from its established role as a GHRH agonist.
Sermorelin and Hypogonadism / Reproductive Endocrinology
Research has explored whether Sermorelin’s GH-stimulating effects may have downstream consequences on the reproductive endocrine axis — specifically, whether enhanced GH and IGF-1 levels may influence gonadotropin release and testosterone production.
In initial animal studies, Sermorelin appeared to stimulate the release of follicle-stimulating hormone (FSH) and luteinizing hormone (LH), the two primary gonadotropins responsible for driving testosterone production in males. These findings prompted further investigation in human subjects.
A subsequent clinical study enrolled 19 male subjects — 9 aged 22–33 and 10 aged 60–78. The elderly subjects received Sermorelin at two concentrations for 28 days each, with a 14-day interval between presentations. While testosterone levels in the elderly subjects reportedly increased following Sermorelin presentation, the investigators noted that the elevations did not reach statistical significance.
An additional observation from this study was that the elevated GH levels potentially stimulated by Sermorelin appeared to peak during nighttime hours across all subjects — consistent with the known circadian pattern of endogenous GH secretion, where the largest natural GH pulses occur during slow-wave sleep. This circadian concordance further supports the characterization of Sermorelin as a GHRH analog that works within the body’s existing physiological rhythms rather than overriding them.
Summary of Key Research Findings
- GH Stimulation — 82% enhancement in average GH levels with effects persisting approximately 2 hours; separate 16-week study showed 107% GH increase and 28% IGF-1 increase
- Receptor Specificity — Stimulates GH via GHRH receptor without significant changes in prolactin, insulin, cortisol, glucose, or thyroid hormones
- Growth Velocity — Increased growth rates within 12 months of presentation in GH deficiency models, sustained for an average of 36 months with continuous presentation.
- Body Composition — 1.26 kg lean mass gain without fat mass change; significant increase in skin thickness (16-week study); reduced visceral fat in HIV-associated lipodystrophy (12-week study)
- Lipodystrophy — Significant reduction in abdominal visceral fat and trunk-to-extremity fat ratio in HIV-positive subjects without glucose or insulin perturbation
- Cognition — Improved performance on WAIS (IQ, picture arrangement, verbal tests) in elderly subjects aged 68–69
- Tumor Research — Highest sensitivity score among 4,000+ compounds tested in 1,018 glioma subjects; proposed mechanism of tumor cell cycle blockade
- Hypogonadism — Stimulated FSH and LH release in animal models; trend toward increased testosterone in elderly male subjects (not statistically significant); GH peaks concordant with circadian sleep rhythm
- Half-Life — Approximately 11–12 minutes; produces pulsatile GH release closely mirroring natural secretion patterns
Handling and Reconstitution
- Store lyophilized powder at -20°C for long-term stability.
- Reconstitute with bacteriostatic water or sterile water for injection.
- Once reconstituted, store at 2–8°C (refrigerator temperature)
- Use the reconstituted solution within 30 days.
- Avoid repeated freeze-thaw cycles.
- Handle with appropriate laboratory safety protocols.
Quality Assurance
- Purity verified at >99% by high-performance liquid chromatography (HPLC)
- Identity confirmed by mass spectrometry (MS)
- Certificate of Analysis (COA) available for every batch
- Third-party tested for purity, identity, and consistency.
- Supplied as lyophilized (freeze-dried) powder for maximum stability
Frequently Asked Questions
What is Sermorelin?
Sermorelin is a synthetic peptide consisting of 29 amino acids that functions as the shortest functional analog of growth hormone-releasing hormone (GHRH). It retains full biological activity at the GHRH receptor despite containing only 29 of the native hormone’s 44 amino acids. It has been extensively studied for GH stimulation, body composition, growth velocity, cognition, lipodystrophy, tumor biology, and reproductive endocrinology.
How is Sermorelin different from CJC-1295?
Both activate the same GHRH receptor and the same cAMP/PKA signaling pathway. The difference is pharmacokinetics. Sermorelin has a half-life of approximately 11–12 minutes and produces brief, pulsatile GH release. CJC-1295 without DAC has a half-life of ~30 minutes. CJC-1295 with DAC has a half-life of ~6–8 days. Sermorelin most closely mimics the body’s natural GH pulsatility.
Was Sermorelin ever FDA-approved?
Yes. Sermorelin was previously FDA-approved as a diagnostic agent for assessing growth hormone deficiency (marketed under the trade name Geref). Its regulatory status has evolved, but it remains one of the most extensively studied GHRH analogs in published clinical literature.
Does Sermorelin affect hormones other than growth hormone?
Research indicates that Sermorelin does not induce significant changes in prolactin, insulin, cortisol, glucose, or thyroid hormone levels — making it one of the most receptor-specific GHRH analogs available for research purposes.
What is the half-life of Sermorelin?
Approximately 11–12 minutes. This positions it between native GHRH (~7 minutes) and modified analogs like CJC-1295 without DAC (~30 minutes). The short half-life produces discrete, pulse-like GH secretion events that closely mirror natural physiological patterns.
What areas of research has Sermorelin been studied in?
Growth hormone stimulation, growth velocity in GH deficiency, body composition and lean mass, HIV-associated lipodystrophy, age-related cognitive decline, glioma tumor cell sensitivity, and hypogonadism/reproductive endocrinology.
Can Sermorelin be combined with other peptides?
Sermorelin is often studied alongside growth hormone secretagogues such as Ipamorelin. Because Sermorelin activates the GHRH receptor (cAMP/PKA pathway) and Ipamorelin activates the ghrelin receptor (PLC/IP3/Ca²⁺ pathway), their simultaneous use may produce synergistic GH release through parallel signaling cascades.
What is the purity of this product?
Greater than 99%, verified by third-party HPLC and mass spectrometry. A Certificate of Analysis is available for every batch.
What size is available?
5mg.
How should I store this product?
Store lyophilized powder at -20°C. Once reconstituted, store at 2–8°C and use within 30 days. Avoid repeated freeze-thaw cycles.
What is this product intended for?
This product is intended for laboratory and research purposes only. It is not intended for human consumption, therapeutic use, or diagnostic purposes.
References
- Garcia, J. M., Merriam, G. R., & Kargi, A. Y. (2019). Growth Hormone in Aging. In K. R. Feingold et al. (Eds.), Endotext. MDText.com, Inc. https://www.ncbi.nlm.nih.gov/books/NBK279163/
- Prakash, A., & Goa, K. L. (1999). Sermorelin: a review of its use in the diagnosis and treatment of children with idiopathic growth hormone deficiency. BioDrugs, 12(2), 139–157. https://pubmed.ncbi.nlm.nih.gov/18031173/
- National Center for Biotechnology Information. PubChem Compound Summary for CID 16129620, Sermorelin. PubChem. https://pubchem.ncbi.nlm.nih.gov/compound/16129620
- Clark, R. G., & Robinson, I. C. (1985). Growth induced by pulsatile infusion of an amidated fragment of human growth hormone-releasing factor in normal and GHRF-deficient rats. Nature, 314(6008), 281–283. https://pubmed.ncbi.nlm.nih.gov/2858818/
- Drugs at FDA: FDA-Approved Drugs. https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=020443
- Junichi, I., et al. (2020). Growth hormone secretagogues: history, mechanism of action, and clinical development. JSCM Rapid Communications, 3(1). https://doi.org/10.1002/rco2.9
- Prakash, A., & Goa, K. L. (1999). Sermorelin: a review of its use in the diagnosis and treatment of children with idiopathic growth hormone deficiency. BioDrugs, 12(2), 139–157. https://pubmed.ncbi.nlm.nih.gov/18031173/
- Koutkia, P., et al. (2004). Growth hormone-releasing hormone in HIV-infected men with lipodystrophy: a randomized controlled trial. JAMA, 292(2), 210–218. https://pubmed.ncbi.nlm.nih.gov/15249570/
- Vitiello, M. V., et al. (2006). Growth hormone-releasing hormone improves cognitive function in healthy older adults. Neurobiology of Aging, 27(2), 318–323. https://pubmed.ncbi.nlm.nih.gov/16399214/
- Chang, Y., et al. (2021). A potentially effective drug for patients with recurrent glioma: sermorelin. Annals of Translational Medicine, 9(5), 406. https://doi.org/10.21037/atm-20-6561
- Sinha, D. K., et al. (2020). Beyond the androgen receptor: the role of growth hormone secretagogues in the modern management of body composition in hypogonadal males. Translational Andrology and Urology, 9(Suppl 2), S149–S159. https://doi.org/10.21037/tau.2019.11.30
- Zhou, F., et al. (2020). Structural basis for activation of the growth hormone-releasing hormone receptor. Nature Communications, 11(1), 5205. https://doi.org/10.1038/s41467-020-18945-0
- Vittone, J., et al. (1997). Effects of single nightly injections of growth hormone-releasing hormone (GHRH 1-29) in healthy elderly men. Metabolism, 46(1), 89–96. https://doi.org/10.1016/s0026-0495(97)90174-8
- Khorram, O., Laughlin, G. A., & Yen, S. S. (1997). Endocrine and metabolic effects of long-term administration of [Nle27]growth hormone-releasing hormone-(1-29)-NH2 in age-advanced men and women. Journal of Clinical Endocrinology & Metabolism, 82(5), 1472–1479. https://doi.org/10.1210/jcem.82.5.3943
Disclaimer
This product is sold for research and laboratory use only. It is not a drug, food, cosmetic, or supplement. It is not intended to diagnose, treat, cure, or prevent any disease or medical condition. It is not approved for human or veterinary use. The information provided on this page is drawn from published preclinical and clinical research literature and is presented for informational purposes only. Researchers are responsible for ensuring compliance with all applicable regulations governing the purchase, handling, and use of research peptides in their jurisdiction.
All products sold by TQ Peptides are intended strictly for laboratory research, analytical testing, and in vitro experimental purposes only. These products are not intended for human or animal consumption.
TQ Peptides operates solely as a research chemical supplier and is not a compounding pharmacy or chemical compounding facility as defined under Section 503A of the Federal Food, Drug, and Cosmetic Act. Additionally, TQ Peptides is not classified as an outsourcing facility under Section 503B of the same Act.
The statements made on this website have not been evaluated by the U.S. Food and Drug Administration (FDA). Products sold by TQ Peptides are not intended to diagnose, treat, cure, or prevent any disease.

