
Product Specifications
- Peptide: Tesamorelin
- Other Designations: TH9507, (3E)-hex-3-enoylsomatoliberin, N-(trans-3-hexenoyl)-[Tyr1]hGRF(1–44)NH₂ acetate
- Classification: A powerful, modified hormone uniquely designed to maximize the body’s own growth hormone release potential.
- Available Sizes: 5mg and 10mg
- Form: Lyophilized (freeze-dried) powder
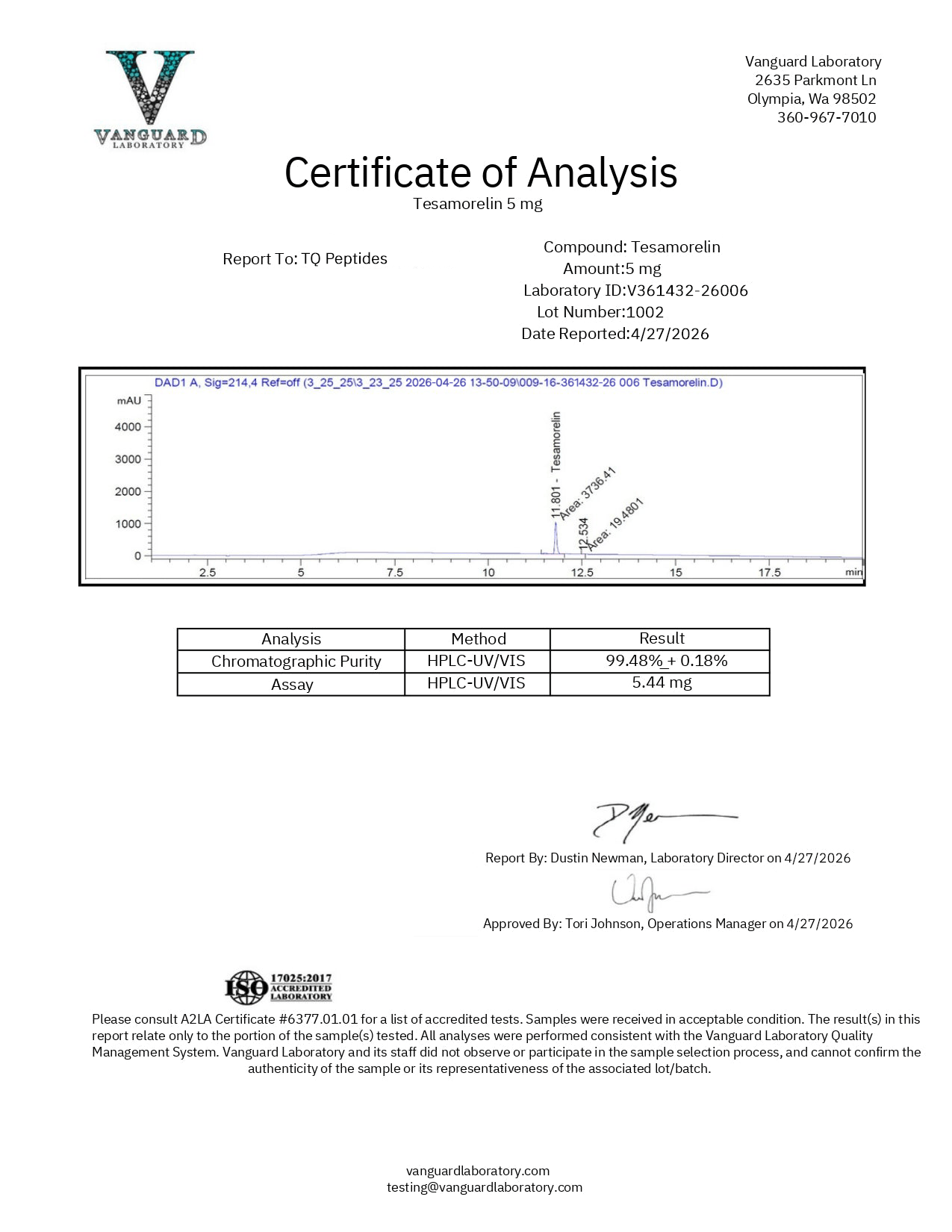
- Purity: >99%
- Amino Acid Count: 44. Tesamorelin matches the length of the natural hormone it’s based on, with modifications at both ends for greater effectiveness and duration.
- Molecular Formula: C₂₂₁H₃₆₆N₇₂O₆₇S
- Molecular Weight: 5136 g/mol
- Receptor Target: Growth Hormone-Releasing Hormone Receptor (GHRH-R)
- Regulatory Status: Tesamorelin is the only GHRH analog with current FDA approval (as Egrifta/Egrifta SV for HIV-associated lipodystrophy), positioning it as the gold standard and the most clinically validated choice in its class.
- Origin: Synthetic. It is a 44-amino-acid modified copy of the natural hormone.
- Storage: Keep the powder frozen at -20°C. After mixing with liquid, refrigerate at 2–8°C and use within 30 days.
- Intended Use: For laboratory and research purposes only. Not for human consumption.
- Third-party tested with Certificate of Analysis available.
What Is Tesamorelin?
Tesamorelin is a synthetic peptide with 44 amino acids. It matches the full-length human GHRH sequence, with changes at both ends to improve stability. Unlike other GHRH analogs, Tesamorelin uses the entire GHRH sequence and is the only one approved by the FDA.
Tesamorelin has two main modifications: a trans-3-hexenoic acid group at one end and an acetyl group at the other. These boost stability and activity, helping Tesamorelin maintain full effectiveness and last longer than the natural hormone.
Like other GHRH analogs in the research catalog, Tesamorelin binds to GHRH receptors on somatotroph cells in the anterior pituitary gland, stimulating growth hormone (GH) secretion and insulin-like growth factor 1 (IGF-1) production. Sermorelin has 29 amino acids and is unmodified; CJC-1295 has 29 amino acids with four substitutions, with or without DAC. Tesamorelin’s uniqueness lies in its full-length sequence, its stabilization at both termini, and its status as the only GHRH analog with FDA approval and confirmed clinical efficacy.
Tesamorelin is available as a premium freeze-dried powder with verified purity of> 99%. Choose between 5mg or 10mg sizes to confidently support your research needs.
How Tesamorelin Works — Proposed Mechanism of Action
Tesamorelin activates GHRH receptors with greater stability, enabling sustained receptor engagement.
Tesamorelin binds to GHRH receptors in the pituitary, triggering a series of steps that increase growth hormone production.
Growth hormone released by Tesamorelin acts mainly on the liver to boost IGF-1 production, which drives cell growth and protein synthesis.
In clinical research, Tesamorelin increased overall GH by 69% and the mean GH pulse area by 55%, without altering GH pulse frequency or peak amplitude. IGF-1 increased by 122%. This amplification of GH pulses without disrupting rhythm reflects the pulsatility-preserving profile of GHRH receptor agonists.
Along with raising GH and IGF-1, Tesamorelin also helps break down stored fat, especially around the abdomen and organs. This mechanism supports its main researched use: reducing harmful visceral fat.
Tesamorelin’s Position in the GHRH Analog Family
Tesamorelin is unique among GHRH analogs for its full-length sequence, double modifications, and clinical approval.
- Native GHRH (1-44) — The natural hormone in the body, with 44 amino acids. It breaks down quickly in the body (about 7 minutes), so it is not often used in research.
- Sermorelin / GRF 1-29 — A shorter piece of the hormone with 29 amino acids. It lasts a little longer (about 11–12 minutes). It was used before to test for growth hormone problems. It is similar to the body’s natural hormone and has been widely studied.
- CJC-1295 without DAC (Mod GRF 1-29) — This is a form of the hormone that is 29 amino acids long and has 4 small changes to help it last longer (about 30 minutes). It still works in bursts inside the body.
- CJC-1295 with DAC — Same base as above, but with an extra group that helps it stick to blood proteins, making it last 6–8 days in the body.
- Tesamorelin is a full-length GHRH analog with terminal modifications for added stability. It is the only one with current FDA approval and is supported by strong clinical trial evidence, including Phase III data.
Tesamorelin uses the complete 44-amino-acid sequence. It fully engages the GHRH receptor, not a truncated approximation. Its dual-terminus modifications give stability without changing the core receptor-binding domain. FDA approval means it passed the strictest regulatory standards for any peptide in this class.
Preclinical and Clinical Research Overview
Tesamorelin boasts one of the strongest clinical evidence portfolios among GHRH analogs, including multiple Phase III trials and ongoing research. Below is a focused summary by research area that illustrates Tesamorelin’s remarkable efficacy and promise.
Tesamorelin and Visceral Fat / Lipodystrophy
Tesamorelin is the primary focus of lipodystrophy research, and its proven efficacy in reducing harmful belly fat is key to its FDA approval.
Lipodystrophy involves abnormal fat distribution — loss of subcutaneous fat in some areas (lipoatrophy) combined with pathological accumulation of visceral fat in others (lipohypertrophy). This condition is associated with serious metabolic consequences, including insulin resistance, elevated triglycerides and cholesterol, and increased cardiovascular risk. Models with lipodystrophy typically exhibit suppressed GH and IGF-1 levels.
In two pivotal Phase III clinical trials, 806 immunodeficient subjects with lipodystrophy were enrolled across a combined 52-week study period. During the first 26 weeks, 543 subjects received Tesamorelin while 263 received a placebo. At week 26, the Tesamorelin group was re-randomized — half continued Tesamorelin and half switched to placebo for an additional 26 weeks.
The results at week 26 were clear: People who took Tesamorelin had at least a 15.4% reduction in deep belly fat compared with those who received a placebo. They also had lower fat (triglyceride) and cholesterol in their blood.
A comprehensive systematic review has shown that Tesamorelin can reduce visceral fat by up to 25%, cementing its position as one of the most potent pharmacological solutions ever studied for pathological fat accumulation.
Tesamorelin and Hepatic Fat / Non-Alcoholic Fatty Liver Disease
An important area of Tesamorelin research is liver fat, focusing on non-alcoholic fatty liver disease, found in nearly 40% of HIV-positive people.
In a randomized, double-blind study, 61 HIV-positive subjects with elevated hepatic fat fraction (HFF) were presented with either Tesamorelin or a placebo for 12 months. The primary endpoint was the rate of change in HFF over the study period.
The results demonstrated a meaningful separation between groups: 35% of Tesamorelin subjects achieved a reduction in hepatic fat fraction below 5% (a clinically significant threshold), compared with only 4% of placebo subjects. Notably, no significant alteration in glucose levels was observed, maintaining the metabolic safety profile that characterizes GHRH receptor agonists.
This NAFLD finding broadens Tesamorelin’s research profile beyond abdominal fat and subcutaneous fat. It suggests Tesamorelin’s GH-driven fat reduction may also affect fat inside organs, not just typical fat deposits.
Tesamorelin and Muscle Tissue Composition
Beyond its effects on fat metabolism, researchers have investigated whether Tesamorelin’s GH-stimulating effects influence muscle tissue quality and composition.
Using computed tomography (CT) imaging, investigators evaluated the structural characteristics of specific muscle groups before and after Tesamorelin presentation. The findings suggested a potential association between Tesamorelin and improvements in both muscle density and muscle volume. Specific muscle groups — including the rectus abdominis, psoas major, and paraspinal muscles — exhibited statistically significant variations compared to placebo controls.
These variations included increased muscle density and volume, and decreased intramuscular fat content. The reduction in fat within muscle tissue is particularly noteworthy — intramuscular fat infiltration is associated with reduced muscle quality, decreased functional capacity, and metabolic dysfunction. By potentially reducing this fat infiltration while simultaneously increasing muscle density, Tesamorelin may offer a dual-action improvement in muscle tissue composition that goes beyond simple hypertrophy.
Tesamorelin and Cognition
An active area of Tesamorelin research examines the peptide’s potential influence on neurocognitive function — specifically in immunodeficient populations with mild cognitive impairment.
A clinical trial enrolled 100 subjects aged 40 or older with immunodeficiency and mild cognitive impairment. The study design involved daily Tesamorelin administration for 6 months, followed by a 6-month washout period (no peptide), and then a second 6-month Tesamorelin administration period. The primary outcome measure was change in neurocognitive performance as measured by the Global Deficit Score (GDS) at 6 and 12 months.
This study follows the same research thread explored with Sermorelin — the hypothesis that age- and disease-related decline in GH and IGF-1 levels may contribute to cognitive impairment, and that restoring GH axis activity through GHRH receptor stimulation may support cognitive function. Tesamorelin’s full-length sequence and enhanced stability make it particularly well-suited for this type of extended-duration cognitive study, where consistent GHRH receptor engagement over months is essential to the experimental design.
Tesamorelin and Insulin Sensitivity
Given that visceral fat accumulation is closely associated with insulin resistance, researchers have investigated whether Tesamorelin’s fat-reducing effects also influence glucose metabolism — and whether the peptide itself introduces any metabolic risks.
In a 12-week randomized clinical trial, 53 subjects with Type II diabetes received either a lower or a higher dose of Tesamorelin or placebo. Investigators measured fasting glucose, glycosylated hemoglobin (HbA1c), and overall diabetes control at the end of the study period.
The results showed no significant reduction in any of these parameters — but critically, no significant worsening either. All three groups produced statistically similar outcomes, leading investigators to conclude that Tesamorelin did not appear to meaningfully alter insulin sensitivity in either direction in this Type II diabetes population.
This finding is considered an important context for Tesamorelin research because it addresses a common concern with GH-axis stimulation: that increased GH levels might worsen insulin resistance. The clinical data suggest that Tesamorelin — even while producing meaningful reductions in visceral fat and elevations in GH and IGF-1 — does not appear to disrupt glucose homeostasis in diabetic subjects. This metabolic neutrality, combined with the NAFLD study showing no glucose alterations and the Phase III trials showing improved lipid profiles, strengthens the characterization of Tesamorelin as a GHRH agonist with a favorable metabolic safety profile.
Tesamorelin Structural Modifications — Why They Matter
Understanding the specific structural modifications that distinguish Tesamorelin from native GHRH is important for researchers comparing it to other GHRH analogs in the class.
C-terminus modification: trans-3-hexenoic acid group. This omega-amino acid modification is attached to the C-terminal end of the peptide. It is believed to reinforce the molecule’s defense against enzymatic breakdown — a critical improvement given that native GHRH is rapidly degraded by dipeptidyl peptidase-4 (DPP-IV) and other serum proteases, resulting in a half-life of only ~7 minutes.
N-terminus modification: acetyl group (CH₃CO-). Acetylation of the N-terminus is believed to enhance both the molecule’s stability and its biological activity. This modification protects the vulnerable N-terminal residue from aminopeptidase attack while potentially improving receptor-binding efficacy.
Comparison to CJC-1295 modifications: CJC-1295 (Mod GRF 1-29) achieves stability through four amino acid substitutions within the peptide chain itself (positions 2, 8, 15, and 27). Tesamorelin takes a different approach — leaving the core 44-amino-acid sequence largely intact and instead adding stabilizing groups at the two termini. This strategy preserves the native GHRH receptor-binding profile while achieving enhanced enzymatic resistance through a fundamentally different chemical strategy.
5mg vs 10mg — Choosing the Right Size
Both sizes contain the identical Tesamorelin peptide at >99% purity. The choice between them depends on the research protocol:
- 5mg — Appropriate for shorter-duration studies, pilot investigations, dose-response assessments, or research protocols with lower total peptide requirements. Lower cost entry point for initial compound evaluation.
- 10mg — Provides greater flexibility for extended study durations, multi-week protocols, higher-concentration reconstitution, or research designs requiring repeated administrations from a single vial. More cost-efficient per milligram for committed, longer-term research.
Both sizes are supplied as lyophilized powder in sealed research vials with full COA documentation.
Summary of Key Research Findings
- GH Elevation — 69% increase in overall GH levels (AUC); 55% increase in mean GH pulse area; natural pulse frequency and peak levels preserved; 122% increase in IGF-1
- Visceral Fat Reduction — At least 15.4% decrease in VAT at 26 weeks in Phase III trials (806 subjects); up to 25% reduction reported in systematic review
- Lipid Profile — Significant decreases in triglyceride and cholesterol levels in lipodystrophy subjects
- Hepatic Fat — 35% of treated subjects achieved <5% hepatic fat fraction vs 4% placebo in a 12-month NAFLD study; no glucose alterations
- Muscle Composition — Increased muscle density and volume in rectus abdominis, psoas major, and paraspinal muscles; decreased intramuscular fat content
- Insulin Safety — No significant alteration in fasting glucose, HbA1c, or diabetes control in Type II diabetes subjects over 12 weeks
- Cognition — Active clinical trial investigating neurocognitive performance (GDS) in immunodeficient subjects with mild cognitive impairment over an 18-month protocol
- FDA Status — The only GHRH analog with current FDA approval, supporting the compound’s clinical evidence base and safety characterization
Handling and Reconstitution
- Store lyophilized powder at -20°C for long-term stability.
- Reconstitute with bacteriostatic water or sterile water for injection.
- Once reconstituted, store at 2–8°C (refrigerator temperature)
- Use the reconstituted solution within 30 days.
- Avoid repeated freeze-thaw cycles.
- The dual-terminus modifications provide enhanced stability compared to native GHRH, but standard peptide-handling protocols should still be followed.
- Handle with appropriate laboratory safety protocols.
Quality Assurance
- Purity verified at >99% by high-performance liquid chromatography (HPLC)
- Identity confirmed by mass spectrometry (MS)
- Certificate of Analysis (COA) available for every batch
- Third-party tested for purity, identity, and consistency.
- Supplied as lyophilized (freeze-dried) powder for maximum stability
- Both 5mg and 10mg sizes were tested to the same quality standard.
Frequently Asked Questions
What is Tesamorelin?
Tesamorelin is a synthetic 44-amino-acid peptide that functions as a full-length analog of growth hormone-releasing hormone (GHRH) with stabilizing modifications at both the N-terminus (acetylation) and C-terminus (trans-3-hexenoic acid). It is the only GHRH analog currently approved by the FDA and has been extensively studied for visceral fat reduction, lipodystrophy, hepatic steatosis, muscle composition, cognition, and insulin safety.
How is Tesamorelin different from Sermorelin?
Both activate the same GHRH receptor and cAMP/PKA signaling pathway. Sermorelin contains 29 amino acids (the shortest functional GHRH fragment) with no structural modifications. Tesamorelin contains the full 44-amino-acid GHRH sequence with dual-terminus stabilization. Tesamorelin binds the GHRH receptor with the full native binding profile and is currently FDA-approved. Sermorelin was previously FDA-approved, but its status has since changed.
How is Tesamorelin different from CJC-1295?
CJC-1295 is a 29-amino-acid truncated fragment with four internal amino acid substitutions (± DAC for extended half-life). Tesamorelin is the full 44-amino-acid sequence with terminal modifications. CJC-1295 with DAC has the longest half-life (~6–8 days) in the class, while Tesamorelin has the most complete clinical evidence base, including Phase III trials and FDA approval.
Is Tesamorelin FDA-approved?
Yes. Tesamorelin is the only GHRH analog currently approved by the FDA. It was approved for the treatment of HIV-associated lipodystrophy and is marketed under the brand names Egrifta and Egrifta SV.
What clinical evidence supports Tesamorelin?
Phase III trials in 806 lipodystrophy subjects showed 15.4%+ visceral fat reduction; a 12-month NAFLD trial showing 35% of subjects achieving <5% hepatic fat; a 12-week diabetes trial confirmed no glucose disruption; CT-based muscle composition studies showed improved density and reduced intramuscular fat; and an ongoing cognition trial in mild cognitive impairment.
Does Tesamorelin affect insulin or glucose?
Clinical research indicates that Tesamorelin does not significantly alter fasting glucose, HbA1c, or insulin sensitivity — even in Type II diabetes subjects and while producing meaningful reductions in visceral and hepatic fat.
How much does Tesamorelin increase GH and IGF-1?
Research reports a 69% increase in overall GH levels (AUC), a 55% increase in mean GH pulse area, and a 122% surge in IGF-1 levels — while preserving the natural frequency and peak amplitude of GH pulses.
What sizes are available?
5mg and 10mg. Both contain identical Tesamorelin at >99% purity. The 5mg suits shorter studies; the 10mg provides more volume for extended or higher-dose protocols.
What is the purity of this product?
Greater than 99%, verified by third-party HPLC and mass spectrometry. A Certificate of Analysis is available for every batch.
How should I store this product?
Store lyophilized powder at -20°C. Once reconstituted, store at 2–8°C and use within 30 days. Avoid repeated freeze-thaw cycles.
What is this product intended for?
This product is intended for laboratory and research purposes only. It is not intended for human consumption, therapeutic use, or diagnostic purposes.
References
- National Institute of Diabetes and Digestive and Kidney Diseases. (2018). Tesamorelin. In Clinical and Research Information on Drug-Induced Liver Injury (LiverTox). https://www.ncbi.nlm.nih.gov/books/NBK548730/
- Spooner, L. M., & Olin, J. L. (2012). Tesamorelin: a growth hormone-releasing factor analog for HIV-associated lipodystrophy. The Annals of Pharmacotherapy, 46(2), 240–247. https://doi.org/10.1345/aph.1Q629
- Stanley, T. L., Chen, C. Y., Branch, K. L., Makimura, H., & Grinspoon, S. K. (2011). Effects of a growth hormone-releasing hormone analog on endogenous GH pulsatility and insulin sensitivity in healthy men. Journal of Clinical Endocrinology & Metabolism, 96(1), 150–158. https://doi.org/10.1210/jc.2010-1587
- Ferdinandi, E. S., Brazeau, P., High, K., Procter, B., Fennell, S., & Dubreuil, P. (2007). Non-clinical pharmacology and safety evaluation of TH9507, a human growth hormone-releasing factor analog. Basic & Clinical Pharmacology & Toxicology, 100(1), 49–58. https://doi.org/10.1111/j.1742-7843.2007.00008.x
- Stanley, T. L., Fourman, L. T., Feldpausch, M. N., et al. (2019). Effects of tesamorelin on non-alcoholic fatty liver disease in HIV: a randomized, double-blind, multicentre trial. The Lancet HIV, 6(12), e821–e830. https://doi.org/10.1016/S2352-3018(19)30338-8
- Falutz, J., Mamputu, J. C., Potvin, D., et al. (2010). Effects of tesamorelin (TH9507), a growth hormone-releasing factor analog, in human immunodeficiency virus-infected patients with excess abdominal fat: a pooled analysis of two multicenter, double-blind, placebo-controlled phase 3 trials with safety extension data. Journal of Clinical Endocrinology & Metabolism, 95(9), 4291–4304. https://doi.org/10.1210/jc.2010-0490
- ClinicalTrials.gov. Tesamorelin Effects on Liver Fat and Histology in HIV. Identifier: NCT02196831. https://clinicaltrials.gov/ct2/show/NCT02196831
- ClinicalTrials.gov. Phase II Trial of Tesamorelin for Cognition in Aging HIV-Infected Persons. Identifier: NCT02572323. https://clinicaltrials.gov/ct2/show/NCT02572323
- Clemmons, D. R., Miller, S., & Mamputu, J. C. (2017). Safety and metabolic effects of tesamorelin, a growth hormone-releasing factor analog, in patients with type 2 diabetes: A randomized, placebo-controlled trial. PLoS ONE, 12(6), e0179538. https://doi.org/10.1371/journal.pone.0179538
- Adrian, S., Scherzinger, A., Sanyal, A., et al. (2019). The Growth Hormone Releasing Hormone Analog, Tesamorelin, Decreases Muscle Fat and Increases Muscle Area in Adults with HIV. Journal of Frailty & Aging, 8(3), 154–159. https://doi.org/10.14283/jfa.2018.45
- Sivakumar, T., Mechanic, O., Fehmie, D. A., & Paul, B. (2011). Growth hormone axis treatments for HIV-associated lipodystrophy: a systematic review of placebo-controlled trials. HIV Medicine, 12(8), 453–462. https://doi.org/10.1111/j.1468-1293.2010.00906.x
Disclaimer
This product is sold for research and laboratory use only. It is not a drug, food, cosmetic, or supplement. It is not intended to diagnose, treat, cure, or prevent any disease or medical condition. It is not approved for human or veterinary use. The information provided on this page is drawn from published preclinical and clinical research literature and is presented for informational purposes only. Researchers are responsible for ensuring compliance with all applicable regulations governing the purchase, handling, and use of research peptides in their jurisdiction.
All products sold by TQ Peptides are intended strictly for laboratory research, analytical testing, and in vitro experimental purposes only. These products are not intended for human or animal consumption.
TQ Peptides operates solely as a research chemical supplier and is not a compounding pharmacy or chemical compounding facility as defined under Section 503A of the Federal Food, Drug, and Cosmetic Act. Additionally, TQ Peptides is not classified as an outsourcing facility under Section 503B of the same Act.
The statements made on this website have not been evaluated by the U.S. Food and Drug Administration (FDA). Products sold by TQ Peptides are not intended to diagnose, treat, cure, or prevent any disease.