
Product Specifications
- Peptide: Thymosin Alpha-1
- Other Designations: TA1, Tα1, Thymalfasin
- Classification: Naturally occurring thymus-derived immunomodulatory peptide
- Available Sizes: 5mg and 10mg
- Form: Lyophilized (freeze-dried) powder
- Purity: >99%
- Amino Acid Count: 28Molecular Formula: C₁₂₉H₂₁₅N₃₃O₅₅
- Molecular Weight: 3101 g/mol
- Precursor Protein: Prothymosin Alpha (113 amino acids)
- Source Gland: Thymus
- Endogenous Origin: Found naturally in Thymosin Fraction 5, which is a basic thymus gland extract
- Primary Research Focus: How it affects the immune system — T-cell growth, NK cell activity, cytokine balance, dendritic cell signals
- Regulatory Context: The lab-made version (Thymalfasin) has been approved in many countries for use in hepatitis B and as an immune support medicine
- Storage: Store lyophilized powder at -20°C. Once reconstituted, store at 2–8°C and use within 30 days.
- Intended Use: For laboratory and research purposes only. Not for human consumption.
- Third-party tested with Certificate of Analysis available.
What Is Thymosin Alpha-1?
Thymosin Alpha-1 holds a unique place among research peptides. It is a naturally occurring immune system peptide with more extensive clinical study than most other peptides available for research. While many peptides have only preclinical data and limited human evidence, Thymosin Alpha-1 has been evaluated in clinical trials for hepatitis B, hepatitis C, sepsis, HIV, and multiple cancer models. Its synthetic form (Thymalfasin) has also received clinical approval in over 35 countries.
The peptide itself is a 28-amino-acid polypeptide derived from the thymus gland — the organ responsible for T-cell maturation and adaptive immune system development. Thymosin Alpha-1 is one of the bioactive components of Thymosin Fraction 5, a crude thymic extract first characterized in the 1960s and 1970s. The naturally occurring peptide is cleaved from a larger 113-amino-acid precursor protein called Prothymosin Alpha.
The thymus gland is most active during childhood and adolescence. After this period, it shrinks and becomes less functional with age. This decline is considered a major driver of immune system aging. As the thymus function fades, so does T-cell production, immune surveillance, and adaptive immune responsiveness—changes that define immunosenescence. Thymosin Alpha-1’s endogenous role is to support T-cell maturation and differentiation in the gland. Its decline with age matches the broader decline in thymic function.
The main research focus of Thymosin Alpha-1 is its immunomodulatory role. It may enhance, restore, and regulate immune function across multiple components of the immune system simultaneously. Studies suggest that this peptide can increase the level of major histocompatibility complex (MHC) class I molecules. It may also stimulate cytokine production, including IL-2, IL-10, and IFN-γ. Thymosin Alpha-1 may enhance natural killer (NK) cell activity, promote T-cell maturation and differentiation, increase high-affinity IL-2 receptors on T lymphocytes, and engage toll-like receptors (TLR-2 and TLR-9) on dendritic cells and other antigen-presenting cells.
Thymosin Alpha-1 acts on T-cells, NK cells, dendritic cells, cytokine networks, and MHC expression. This broad immunomodulatory profile makes it one of the most versatile immune-focused peptides in the research catalog.
Available in 5mg and 10mg sizes. The 5mg size is suited for initial or smaller-scale studies. The 10mg size is suitable for extended or higher-volume research protocols.
How Thymosin Alpha-1 Works — Proposed Mechanisms of Action
Thymosin Alpha-1 is proposed to modulate the immune system through several interconnected mechanisms that collectively enhance both innate and adaptive immune responses.
T-Cell Maturation and Differentiation. This is the foundational mechanism. Thymosin Alpha-1 is proposed to help immature thymocytes in the thymus become mature, functional T-cells. It may specifically target T-helper and cytotoxic T-cell populations, thereby supporting the terminal differentiation of blood lymphocytes into cells capable of launching targeted immune responses. This T-cell maturation function mirrors the role of the thymus gland. Thus, Thymosin Alpha-1 acts as a molecular proxy for thymic activity.
MHC Class I Upregulation. Research has suggested that Thymosin Alpha-1 may increase the surface expression of major histocompatibility complex (MHC) class I molecules on cells. MHC class I molecules are the structures through which cells present intracellular antigens (including viral proteins and tumor-associated antigens) to cytotoxic T-cells. Upregulating MHC class I expression can make infected or abnormal cells more visible to the immune system — effectively “flagging” them for T-cell-mediated destruction.
Natural Killer Cell Enhancement. The peptide may increase natural killer (NK) cell activity. NK cells are innate immune cells that offer rapid, nonspecific defense against virus-infected and tumor cells. This NK cell enhancement provides an extra layer of innate immune surveillance alongside adaptive T-cell responses.
Toll-Like Receptor Engagement. Thymosin Alpha-1 has been proposed to interact with toll-like receptors TLR-2 and TLR-9 on dendritic cells and other antigen-presenting cells. These receptors are pattern-recognition molecules that detect pathogen-associated molecular patterns and initiate innate immune cascades. By engaging TLRs on dendritic cells, Thymosin Alpha-1 may stimulate cytokine production, including IL-2, IL-10, and IFN-γ — signaling molecules that bridge the innate and adaptive immune systems.
Cytokine Modulation. Thymosin Alpha-1 seems to modulate cytokine production rather than simply stimulate it. Research suggests it may increase protective cytokines, such as IL-2 and IFN-γ, and reduce inflammatory cytokines, such as TNF-α, in some inflammatory settings. This ability to boost immune activation when needed, while limiting harmful inflammation, makes it more than just a stimulant. Instead, it is an immunomodulator.
IL-2 Receptor Expression. Thymosin Alpha-1 may increase the expression of high-affinity receptors for interleukin-2 on T lymphocytes. IL-2 is the primary growth factor for T cells, and increasing its receptor density could lead to more vigorous T-cell activation, proliferation, and effector function in response to immune challenges.
Preclinical and Clinical Research Overview
Thymosin Alpha-1 has been investigated across a wide range of immune-related research domains. Below is a detailed summary organized by study focus.
Thymosin Alpha-1 and Hepatitis B / Hepatitis C
The most clinically advanced application of Thymosin Alpha-1 research involves viral hepatitis — particularly hepatitis B and hepatitis C.
In hepatitis B studies, subjects receiving Thymosin Alpha-1 twice weekly for the study duration exhibited a reported virological response rate increase of 40.6%. This finding contributed to the regulatory approval of the synthetic form (Thymalfasin) for the treatment of hepatitis B in multiple countries.
For hepatitis C, the results were more nuanced: subjects appeared to have improved outcomes when Thymosin Alpha-1 was combined with interferon-alpha rather than as a standalone intervention. This combination approach leveraged Thymosin Alpha-1’s immunomodulatory properties alongside interferon’s direct antiviral activity.
The proposed mechanism in hepatitis models involves Thymosin Alpha-1’s engagement with TLR-2 and TLR-9 on dendritic cells, initiating cytokine cascades (IL-2, IL-10, IFN-γ) that support the adaptive immune system’s ability to recognize and target virus-infected hepatocytes. Additionally, the peptide’s potential to reduce inflammatory cytokines, such as TNF-α, may help control hepatic inflammation that accompanies chronic viral infection.
Thymosin Alpha-1 and Sepsis
Sepsis — a life-threatening condition characterized by dysregulated immune response to infection — represents one of the most critical research applications for Thymosin Alpha-1.
A 2015 meta-analysis evaluated 12 controlled clinical trials to assess the peptide’s potential in sepsis. Across the pooled data, researchers observed a significant decline in mortality rate among subjects receiving Thymosin Alpha-1. Subsequent systematic reviews supported the hypothesis that Thymosin Alpha-1 could alleviate the immunosuppression associated with severe sepsis.
The sepsis research context is particularly relevant because sepsis involves a biphasic immune response: an initial hyperinflammatory phase followed by profound immunosuppression. Thymosin Alpha-1’s dual capacity — enhancing immune activation while modulating excessive inflammation — makes it theoretically well-suited for this biphasic dynamic. However, researchers have noted that the peptide’s efficacy may be highly dependent on the timing of administration relative to the sepsis phase, and further investigation is needed to establish optimal timing protocols.
The meta-analyses were conducted on relatively small subject pools, and researchers have called for larger, multicenter trials to confirm the mortality-reduction findings with greater statistical power.
Thymosin Alpha-1 and HIV / Immune Reconstitution
A randomized phase II open-label clinical trial examined Thymosin Alpha-1’s potential to augment immune reconstitution in 20 HIV-positive subjects already receiving highly active antiretroviral therapy (HAART).
Thirteen subjects received Thymosin Alpha-1 twice weekly for 12 weeks, while 7 received a placebo. CD4/CD8 cell counts, CD45 levels, and signal joint T-cell receptor excision circles (sjTREC) levels were monitored every two weeks.
The results revealed an important nuance. CD4, CD8, and CD45 levels did not change significantly in either group. However, sjTREC levels — a marker of recent thymic output and new T-cell production — increased in the Thymosin Alpha-1 group. This elevation suggested that the peptide may have stimulated thymopoiesis (the production of new T cells by the thymus), even though total T-cell numbers and naive/memory T-cell proportions remained unchanged over the study period.
This finding — increased thymic output without corresponding changes in circulating T-cell numbers — suggests that Thymosin Alpha-1’s effects on immune reconstitution may require longer observation periods to translate thymic production into measurable changes in peripheral T-cell populations.
Thymosin Alpha-1 and Cancer Cell Research
Thymosin Alpha-1 has been studied in cancer cell models, with findings suggesting a differential effect depending on cell type—a property shared with GHK-Cu but operating through a distinct mechanism.
In liver carcinoma research, Thymosin Alpha-1 was presented to mice bearing hepatic tumors. Analysis of isolated cells revealed a bifurcated response: reactive oxygen species (ROS) levels were significantly elevated in immune cells (leukocytes), while they were reduced in tumor cells (HepG2). Correspondingly, leukocyte-monocyte levels increased, while HepG2 cell cycle progression was delayed, reducing tumor cell proliferation.
At the molecular level, the study examined the Akt signaling pathway — a cascade known to be influenced by ROS and associated with cell survival and proliferation. In HepG2 cancer cells, Thymosin Alpha-1 exposure was associated with dephosphorylation of Akt at Ser473, indicating decreased Akt activity linked to reduced oxidative stress. This Akt dephosphorylation may underpin the anti-proliferative effect observed in the cancer cell population.
A separate laboratory study investigated Thymosin Alpha-1’s effects on A549 lung cancer cells. The findings suggested several notable actions: anti-proliferative effects at concentrations of 24 and 48 μg/mL (reducing cell viability after 24 hours), enhanced activity of antioxidant enzymes including catalase, superoxide dismutase (SOD), and glutathione peroxidase (GPx), concentration-dependent inhibition of A549 cell migration in scratch assays, and reduction in cellular ROS levels.
Taken together, the cancer cell research suggests that Thymosin Alpha-1 may act through a dual mechanism: directly reducing cancer cell proliferation and migration while simultaneously enhancing the immune system’s ability to surveil and respond to tumor cells — a combination of direct anti-tumor activity and immunological anti-tumor support.
Thymosin Alpha-1 and Immune Cell Activity — Detailed Findings
While the immune-modulating potential of Thymosin Alpha-1 is well established in the literature, one early clinical study provides important context on the variability of individual responses.
In a study of 11 subjects with different immune system dysfunctions, researchers evaluated the levels of natural killer (NK) cells and lymphokine-activated killer (LAK) cells before and after Thymosin Alpha-1 presentation. The immunodeficient subjects demonstrated a mean LAK-cell activity of approximately 65% compared to controls. Following Thymosin Alpha-1 delivery, only 3 of 11 subjects showed improved LAK-cell activity (up to 30%), while the others showed no significant change.
This finding is notable because it demonstrates that Thymosin Alpha-1’s immunomodulatory effects are not uniform across all individuals or all types of immune dysfunction. The peptide’s efficacy appears to depend on the specific nature and severity of the immune impairment, which has implications for research protocol design and subject selection.
Thymosin Alpha-1 in the Context of Thymic Biology
Understanding where Thymosin Alpha-1 fits within the broader biology of the thymus gland helps contextualize its research applications.
The thymus is a specialized lymphoid organ located behind the sternum that serves as the primary site for T-cell maturation. Bone marrow-derived progenitor cells migrate to the thymus, where they undergo a complex selection process that produces mature, immunocompetent T-cells capable of distinguishing self from non-self. The thymus achieves peak function during puberty and then progressively involutes — a process called thymic involution — that reduces the gland’s T-cell production capacity over the following decades.
Thymic involution is considered one of the hallmarks of immune system aging (immunosenescence). The progressive decline in naive T-cell production, reduced T-cell receptor diversity, and impaired adaptive immune responses that characterize aging are all linked to diminished thymic function.
Thymosin Alpha-1 is one of several bioactive peptides originally isolated from the thymus gland. Its role as a T-cell maturation and differentiation factor positions it as a molecular representative of thymic function — a compound whose activity mirrors, in part, the immunological role of the organ from which it was derived. Research interest in restoring or supplementing Thymosin Alpha-1 levels is driven by the hypothesis that exogenous administration of this thymic peptide may partially compensate for the reduced thymic output associated with aging and disease.
5mg vs 10mg — Choosing the Right Size
Both sizes contain identical Thymosin Alpha-1 at>99% purity. The choice depends on the research protocol:
- 5mg — Suited for shorter-duration studies, initial compound evaluation, dose-response assessment, or protocols with lower total peptide requirements.
- 10mg — Provides greater flexibility for extended studies, multi-week protocols, higher-volume reconstitution, or research designs requiring repeated administrations. More cost-efficient per milligram for committed, longer-term research.
Summary of Key Research Findings
- T-Cell Maturation — Stimulates differentiation of thymocytes into mature T-cells; targets T-helper and cytotoxic T-cell populations
- MHC Class I — Upregulates MHC class I expression, improving immune system visibility of infected or abnormal cells
- NK Cell Enhancement — Enhances natural killer cell activity for innate immune surveillance.
- TLR Engagement — Interacts with TLR-2 and TLR-9 on dendritic cells, initiating cytokine cascades (IL-2, IL-10, IFN-γ)
- Hepatitis B — 40.6% increase in virological response rate with twice-weekly presentation; contributed to regulatory approval of Thymalfasin in 35+ countries.
- Hepatitis C — Improved outcomes when combined with interferon-alpha compounds
- Sepsis — Meta-analysis of 12 trials showed significant mortality rate reduction; dual immunomodulatory properties suited for biphasic sepsis dynamics
- HIV — Increased sjTREC levels (thymic output marker) in HAART-treated subjects without changes in total T-cell counts; suggests thymopoiesis stimulation
- Cancer Cells — Differential ROS modulation: increased in immune cells, decreased in liver carcinoma cells; anti-proliferative and anti-migratory effects in lung cancer cells; Akt dephosphorylation in HepG2 cells.
- Antioxidant Enzymes — Enhanced catalase, SOD, and GPx activity in cancer cell models
- Regulatory Status — Synthetic form (Thymalfasin) approved in 35+ countries for hepatitis B and as an immune adjuvant
Handling and Reconstitution
- Store lyophilized powder at -20°C for long-term stability.
- Reconstitute with bacteriostatic water or sterile water for injection.
- Once reconstituted, store at 2–8°C (refrigerator temperature)
- Use the reconstituted solution within 30 days.
- Avoid repeated freeze-thaw cycles.
- Handle with appropriate laboratory safety protocols.
Quality Assurance
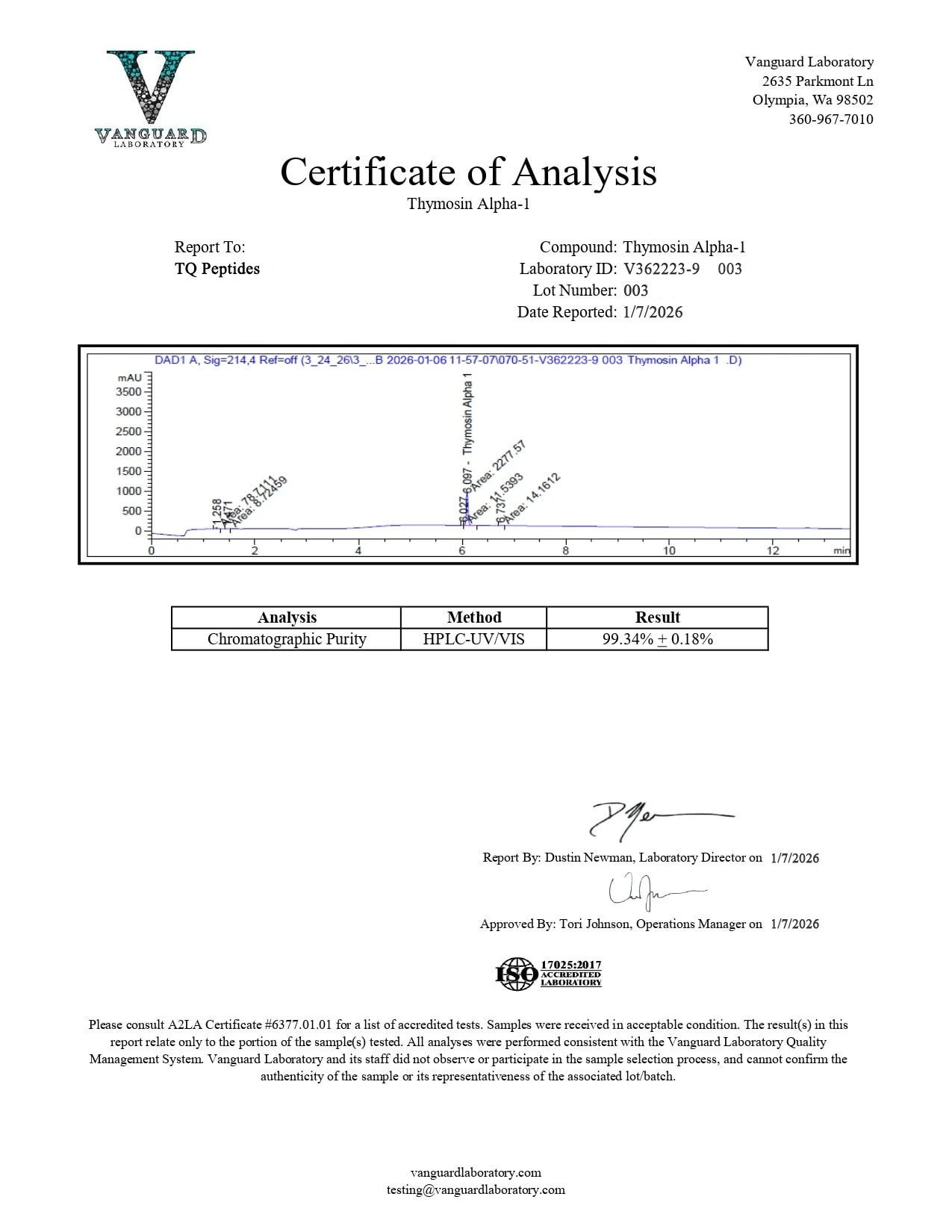
- Purity verified at >99% by high-performance liquid chromatography (HPLC)
- Identity confirmed by mass spectrometry (MS)
- Certificate of Analysis (COA) available for every batch (separate COAs for 5mg and 10mg sizes)
- Third-party tested for purity, identity, and consistency.
- Supplied as lyophilized (freeze-dried) powder for maximum stability
- Both 5mg and 10mg sizes were tested to the same quality standard.
Frequently Asked Questions
What is Thymosin Alpha-1?
Thymosin Alpha-1 (TA1/Tα1) is a naturally occurring 28-amino-acid immunomodulatory peptide derived from the thymus gland. It is cleaved from a 113-amino-acid precursor protein called Prothymosin Alpha. It has been studied for T-cell maturation, NK cell enhancement, cytokine regulation, hepatitis, sepsis, HIV immune reconstitution, and cancer cell research. Its synthetic form (Thymalfasin) is approved in over 35 countries.
What makes Thymosin Alpha-1 different from other peptides?
Two key distinctions. First, it is one of the most clinically studied peptides available for research, with clinical trial data across hepatitis B, hepatitis C, sepsis, HIV, and cancer models. Second, its synthetic form has received regulatory approval in over 35 countries, providing it with a level of clinical validation that most research peptides lack.
What is the thymus gland?
A specialized lymphoid organ located behind the sternum that serves as the primary site for T-cell maturation. It achieves peak function during puberty and then progressively involutes with age, contributing to the decline in adaptive immune function known as immunosenescence.
What is Thymalfasin?
The synthetic version of Thymosin Alpha-1 is identical in amino acid sequence to the naturally occurring peptide. Thymalfasin has been approved for clinical use in over 35 countries, primarily for the treatment of hepatitis B and as an immune adjuvant.
What clinical evidence supports Thymosin Alpha-1?
Hepatitis B: 40.6% virological response rate increase. Sepsis: meta-analysis of 12 trials showing significant mortality reduction. HIV: increased thymic output markers (sjTREC) in HAART-treated subjects. Cancer: anti-proliferative effects in liver carcinoma and lung cancer cell models with differential ROS modulation.
Does Thymosin Alpha-1 work the same in everyone?
No. A clinical study of 11 immunodeficient subjects showed that only 3 exhibited improved LAK-cell activity, while others showed no significant change. The peptide’s efficacy appears to depend on the specific nature and severity of immune impairment.
What sizes are available?
5mg and 10mg. Both contain identical Thymosin Alpha-1 at >99% purity.
What is the purity of this product?
Greater than 99%, verified by third-party HPLC and mass spectrometry. Certificates of Analysis are available for both the 5mg and 10mg sizes.
How should I store this product?
Store lyophilized powder at -20°C. Once reconstituted, store at 2–8°C and use within 30 days. Avoid repeated freeze-thaw cycles.
What is this product intended for?
This product is intended for laboratory and research purposes only. It is not intended for human consumption, therapeutic use, or diagnostic purposes.
References
- Pickart, L., & Margolina, A. (2018). Regenerative and Protective Actions of the GHK-Cu Peptide in the Light of the New Gene Data. International Journal of Molecular Sciences, 19(7), 1987. (Referenced for immunodeficiency context)
- Dominari, A., et al. (2020). Thymosin alpha 1: A comprehensive review of the literature. World Journal of Virology, 9(5), 67–78. https://doi.org/10.5501/wjv.v9.i5.67
- National Center for Biotechnology Information. PubChem Compound Summary for CID 16130571, Thymalfasin. https://pubchem.ncbi.nlm.nih.gov/compound/Thymalfasin
- Garaci, E. (2007). Thymosin alpha1: a historical overview. Annals of the New York Academy of Sciences, 1112, 14–20. https://doi.org/10.1196/annals.1415.039
- Eckert, K., Schmitt, M., Garbin, F., Wahn, U., & Maurer, H. R. (1994). Thymosin alpha 1 effects, in vitro, on lymphokine-activated killer cells from patients with primary immunodeficiencies: preliminary results. International Journal of Immunopharmacology, 16(12), 1019–1025. https://doi.org/10.1016/0192-0561(94)90081-7
- Li, C., Bo, L., Liu, Q., & Jin, F. (2015). Thymosin alpha1-based immunomodulatory therapy for sepsis: a systematic review and meta-analysis. International Journal of Infectious Diseases, 33, 90–96. https://doi.org/10.1016/j.ijid.2014.12.032
- Chadwick, D., et al. (2003). A pilot study of the safety and efficacy of thymosin alpha 1 in augmenting immune reconstitution in HIV-infected patients with low CD4 counts taking highly active antiretroviral therapy. Clinical and Experimental Immunology, 134(3), 477–481. https://doi.org/10.1111/j.1365-2249.2003.02331.x
- Qin, Y., Chen, F. D., Zhou, L., Gong, X. G., & Han, Q. F. (2009). The proliferative and anti-proliferative effects of thymosin alpha1 on cells are associated with modulation of cellular ROS levels. Chemico-Biological Interactions, 180(3), 383–388. https://doi.org/10.1016/j.cbi.2009.05.006
- Kharazmi-Khorassani, J., & Asoodeh, A. (2019). Thymosin alpha-1, a natural peptide, inhibits cellular proliferation, cell migration, and the level of reactive oxygen species and promotes the activity of antioxidant enzymes in the human lung epithelial adenocarcinoma cell line (A549). Environmental Toxicology, 34(8), 941–949. https://doi.org/10.1002/tox.22765
Disclaimer
This product is sold for research and laboratory use only. It is not a drug, food, cosmetic, or supplement. It is not intended to diagnose, treat, cure, or prevent any disease or medical condition. It is not approved for human or veterinary use. The information provided on this page is drawn from published preclinical and clinical research literature and is presented for informational purposes only. Researchers are responsible for ensuring compliance with all applicable regulations governing the purchase, handling, and use of research peptides in their jurisdiction.
All products sold by TQ Peptides are intended strictly for laboratory research, analytical testing, and in vitro experimental purposes only. These products are not intended for human or animal consumption.
TQ Peptides operates solely as a research chemical supplier and is not a compounding pharmacy or chemical compounding facility as defined under Section 503A of the Federal Food, Drug, and Cosmetic Act. Additionally, TQ Peptides is not classified as an outsourcing facility under Section 503B of the same Act.
The statements made on this website have not been evaluated by the U.S. Food and Drug Administration (FDA). Products sold by TQ Peptides are not intended to diagnose, treat, cure, or prevent any disease.